



The target blood pressure level continues to be a topic of ongoing discussion and debate. Hypertension specialists and experts have differing opinions, and panelists of guideline committees have made differing recommendations. Some call for a unique blood pressure target. Michel Burnier, MD, Center Hospital University Vaudois, Lausanne, Switzerland, tackled this topic ESH 2016.
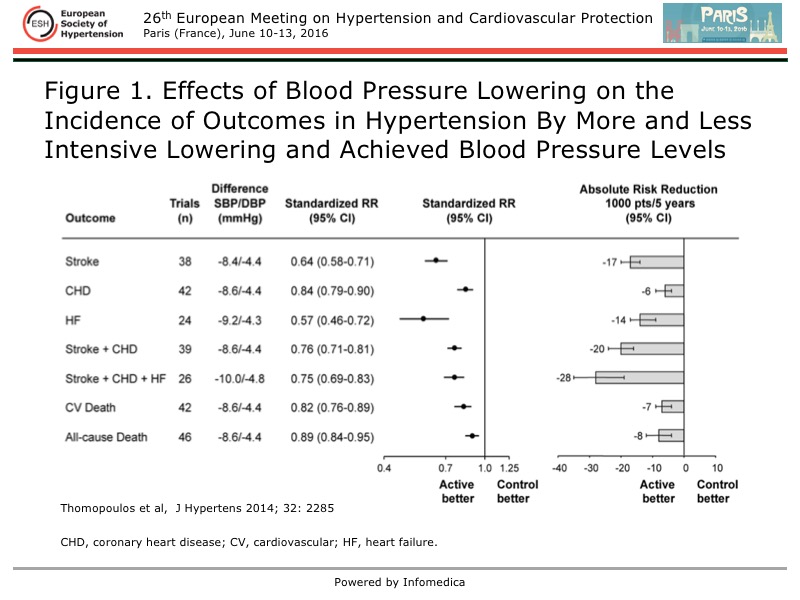
Treatment of hypertension is having a beneficial impact. Age- and sex-adjusted absolute cardiovascular (CV) mortality has been reduced since the 1980s, according to a Euro Heart Survey by the European Society of Cardiology. Randomized, controlled trials of blood pressure lowering have shown that a reduction of 10/5 mmHg produces a reduction in the absolute and relative risk of CV outcomes, including stroke, coronary heart disease, heart failure, CV death, and all-cause death [Thomopoulos C et al. J Hypertens 2016].
However, Burnier noted that the absolute risk reduction found in this meta-analysis of clinical trials was small with little difference compared with the relative risk reduction (Figure 1). Although the substantial impact on CV outcomes from blood pressure lowering is clear, this meta-analysis also showed that stroke was the only outcome for which there was a greater absolute risk reduction by lowering blood pressure to lower levels (130-139 mmHg, <130 mmHg).
{kind=link}
Setting lower blood pressure targets requires evaluating the impact on other factors. What is the price that is paid for more intensive blood pressure lowering to lower targets? Too often, the price is more discontinuation of therapy because of the higher rate of adverse events that occur with more intensive therapy. A key concern is that the patients who are the highest risk of CV events will pay the greatest price of discontinuing treatment, because they are not protected and are at risk of an event.
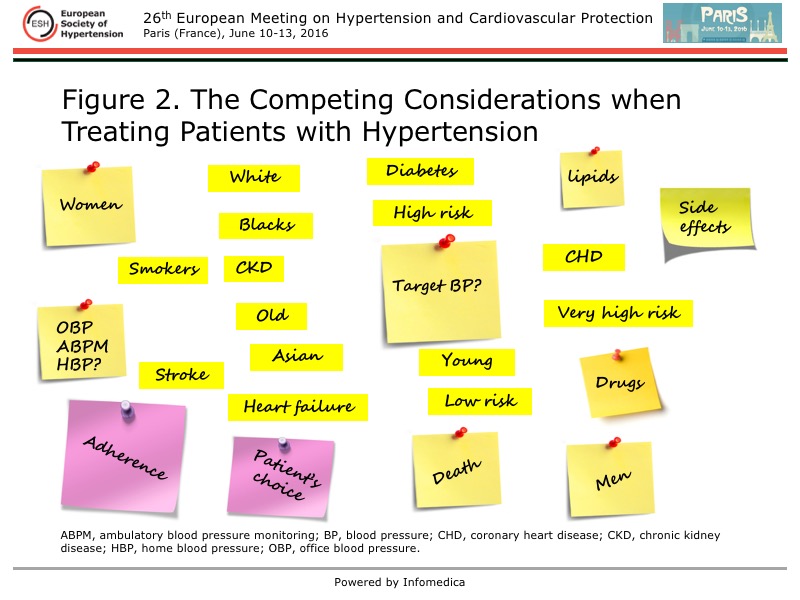
The capacity to achieve in real-world clinical practice the same level of blood pressure lowering as in clinical trials must also be considered. In clinical practice, hypertension is not being treated in isolation, but usually as one of many conditions, such as elevated lipids or diabetes. Moreover, all practice guidelines are advocating lower targets, adding the complexity of treatment. A myriad of competing factors must be balanced by the physician in treating hypertension, some of which are illustrated in Figure 2, and complicate the ability to achieve the target blood pressure. Risk calculation is not always straightforward, limiting easy identification of the patients who warrant more intensive treatment.
{kind=link}
The poor control rates with current targets for blood pressure, as well as for diabetes and lipids, must be recognized. A recent survey of primary care practices in Switzerland showed that only 51% of patients had blood pressure controlled to <140/90 mmHg and only 30% controlled to <130/80 mmHg. Of note, only 2.2% of the patients had all three parameters controlled at goal levels. The low rates of control are the norm around the world. Worldwide, only 32.5% of treated hypertensives had blood pressure control <140/90 mmHg [Chow CK et al. JAMA 2013].
Therefore, Burnier stated the focus should be clear, simple goals that are understandable by health professionals and by patients. Blood pressure targets should be balanced in regard to benefits and risks. Most importantly, the objective should be bringing the maximum number of patients with hypertension to levels <140/90 mmHg, before there is discussion about lower targets set.
Stating that the unique office blood pressure target should <140/90 mmHg, Burnier advocated supporting initiatives aimed at increasing the proportion of patients with controlled hypertension, such as the SIIA initiative working to gain control in 70% of the Italian population and the OBJECTIF 2015 initiative in France that has the same goal.