





An observational study of older adults with cognitive impairment has shown that high-normal levels of systolic blood pressure (SBP) of 130-145 mmHg may be the optimal target to reduce the progression of cognitive decline and reduce the risk of mortality at 3 years. The results were presented by Chiara Lorenzi, MD, AOU, University of Florence, Italy.
This group had recently reported that tight blood pressure control in older adults with cognitive impairment and treated with antihypertensive medications could lead to a greater short-term reduction in decline of cognitive impairment [Mossell E et al. JAMA Intern Med 2015].
Such studies are needed because of the scarce and contradictory data on the prognostic role of high blood pressure in this population. Many studies have demonstrated that high blood pressure can increase the incidence of dementia. Yet, the relation between blood pressure and cognitive impairment remains complex.
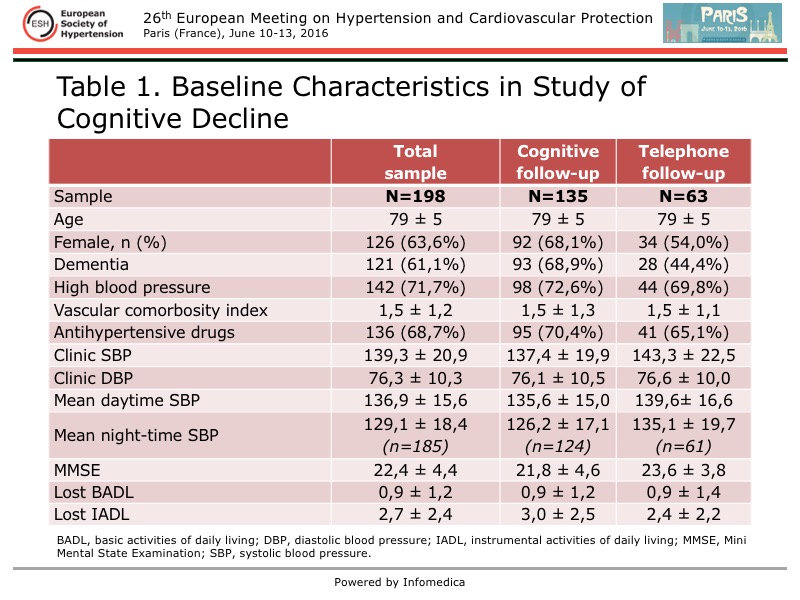
In the present study, Lorenzi and colleagues followed 198 patients to evaluate the 3-year association between clinic blood pressure (CBP), ambulatory blood pressure monitoring (ABPM), and antihypertensive medications. A total of 135 patients, of whom 68.9% had dementia at baseline, underwent cognitive follow-up at baseline and 3 years. The mean age was 79 years, most were women, and 71% had high blood pressure. The baseline characteristics are detailed in Table 1.
{kind=link}
Evaluations conducted in the patients at baseline and 3 years were the Mini Mental State Examination (MMSE) of cognitive status and the Vascular Comorbidity Index, which included high blood pressure, diabetes, heart failure, ischemic heart disease, arrhythmia, stroke/transischemic attack, and kidney disease.
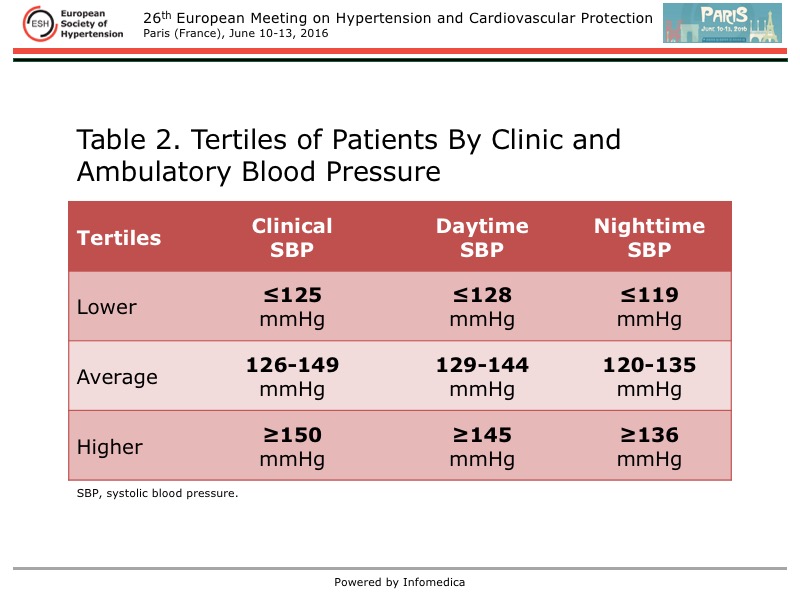
Based on CBP and ABPM, patients were divided into tertiles of blood pressure (Table 2).
{kind=link}
Regarding mortality at 3 years, no association was found between clinic SBP and the event rate across the tertiles. However, a higher rate of morality was found in patients with a higher mean nighttime SBP, both in those treated with antihypertensive drugs (p=0.005) and not treated (p=0.008). A higher mean daytime SBP was also associated with higher mortality, but was not statistically significant.
The association between the higher nighttime SBP and mortality was independent, after adjustments for age, sex, functional status, and cognitive status.
Cognitive outcomes were not associated with clinical blood pressure. But, at 3 years, there was greater progression in cognitive decline in patients with a lower mean SBP (p=0.029). Although a similar trend was seen for lower mean nighttime SBP and progression in cognitive decline, it did not reach statistical significance.
Of note, there was an association between treatment with an antihypertensive medication and greater progression in cognitive decline with a lower mean daytime SBP (p=0.002) and lower mean nighttime SBP (p=0.033), compared with those patients not treated.
The multivariable analysis confirmed an independent association between a lower daytime systolic blood pressure and progression of cognitive decline (p=0.026).
These results showed that a higher mean SBP, especially at night, was prognostic for 3-year mortality, and a lower mean daytime SBP in patients treated with antihypertensive drugs was associated with progression of cognitive impairment. Studies with larger populations are required to confirm these findings. Lorenzi recommends ABPM be used in this vulnerable population.