



The examination of central hemodynamics in patients with hypertension and diabetes, compared without diabetes, revealed a relation between some hemodynamic parameters and diastolic function in work by Davide Agnoletti, MD, Sacro Cuore Hospital, Verona, Italy, and colleagues.
Arterial stiffness is accelerated in the setting of hypertension and diabetes. Previous work by Agnoletti and colleagues has shown that the patterns of pulse wave velocity are different in the setting of diabetic hypertension versus hypertension, with mean arterial pressure not being a significant determinant of pulse wave velocity in diabetic hypertension [Agnoletti D et al. Atherosclerosis 2013]. Other work studying parameters of arterial stiffness and wave reflection found a significant relation between some parameters and indices of diastolic function in men and women [Russo C et al. Hypertension 2012]. However, there was no relation between the amplification of pulse pressure or the augmentation index and diastolic function in men or women.
Therefore, to investigate the relation between diastolic function and arterial hemodynamics in diabetic and nondiabetic hypertension, this group studied 123 patients who had undergone screening for primary or secondary cardiovascular prevention at the Hotel-Dieu Hospital in Paris, France. There was an 89% prevalence of hypertension in this population.
The study patients had ≥1 cardiovascular risk factor. Hemodynamics were measured centrally with tonometry and peripherally, and diastolic function was evaluated with echocardiography. Secondary hypertension, atrial fibrillation, and severe heart failure were exclusion criteria.
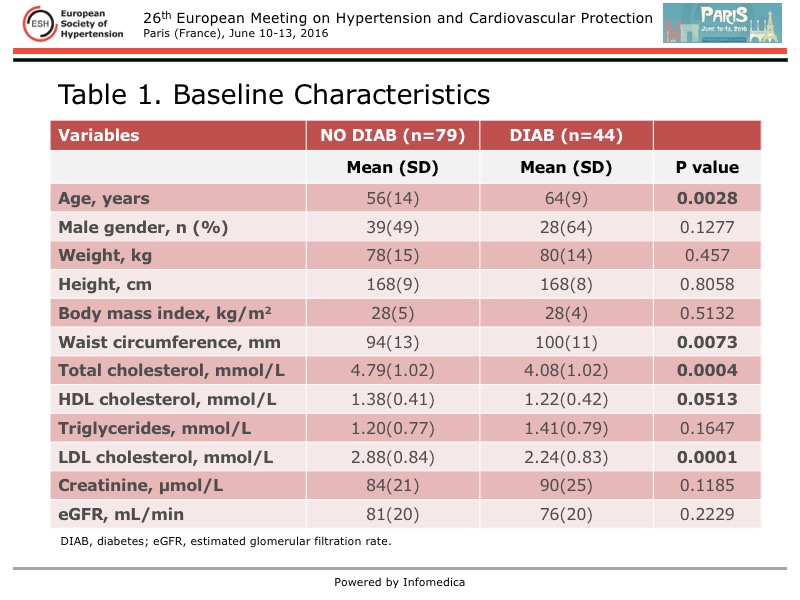
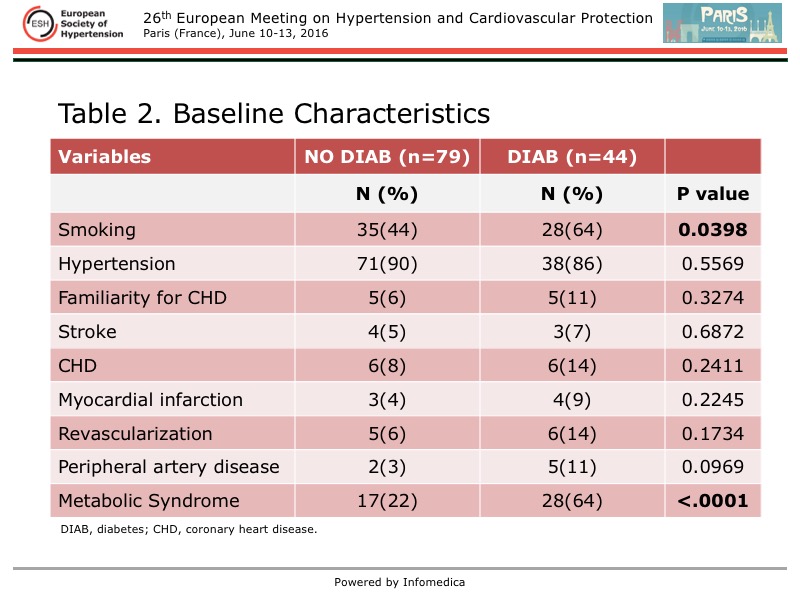
The patients with diabetes were older than those without, but they had a better lipid profile (Table 1 and Table 2). No difference in renal function was seen between the groups. Significantly more patients with diabetic hypertension were smokers and had metabolic syndrome, but the incidence of other comorbidities was similar.
{kind=link}
{kind=link}
More commonly, patients with diabetic hypertension were treated with angiotensin-receptor blockers (nearly 70% vs 20% no diabetes; p<0.05), and less commonly they were treated with calcium channel blockers (about 35% vs 65%; p<0.05).
At baseline, the peripheral and central blood pressures were similar in the two groups. Brachial systolic and diastolic blood pressure (SBP, DBP) was 160 mm Hg and about 90 mm Hg and pulse pressure about 60 mm Hg. Aortic SBP was about 155 mm Hg, DBP about 90 mm Hg, and pulse pressure about 45 mm Hg.
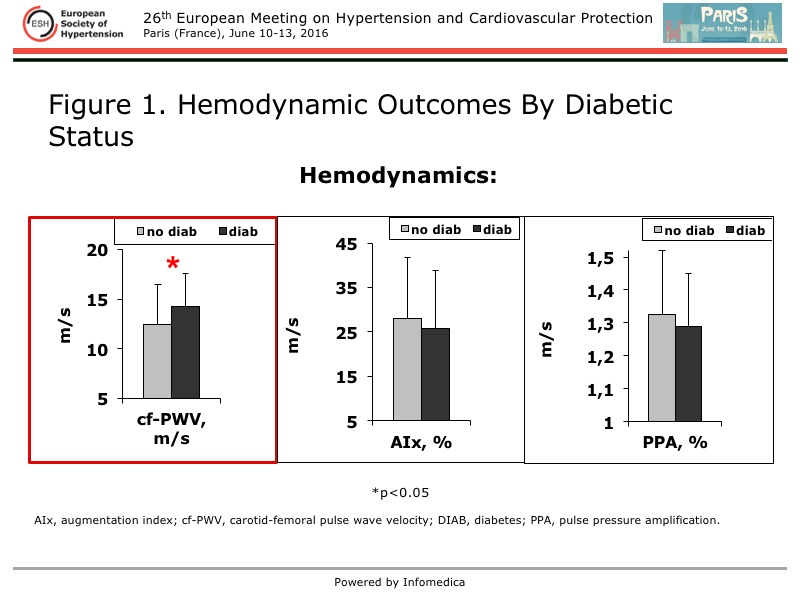
In diabetic hypertension, carotid-femoral pulse wave velocity was significantly higher, but the augmentation index and pulse pressure amplification were similar in the two groups (Figure 1).
{kind=link}
Also similar in diabetic and nondiabetic hypertension was the diastolic and systolic function as evaluated with cardiac ultrasound. The mean left ventricular mass index was 95.3 vs 92.3 g/m2, ejection fraction 67.8% vs 69.2%, E’ wave 9.2 vs 9.4 cm/sec, E/A 0.86 vs 1.01, and the E/e’ was 8.6 vs 8.8, respectively.
In the total population, a significant and positive relation was found between pulse wave velocity and the E/E’ ratio (r=0.199; p=0.027). However, when adjusted for age, sex, mean arterial pressure, and heart rate, no difference was observed in relation to diabetic status. In contrast, the relation between pulse pressure amplification and the E/E’ ratio differed by diabetic status, adjusted for age, sex, mean arterial pressure, and heart rate (p for interaction 0.007). A negative and significant relation was found between pulse pressure amplification and the E/E’ ratio in the total population (r=0.172; p=0.057) and in those with diabetes (r=0.352; p=0.019), but not in those without diabetes (r=0.108; p=0.343).
The determinants of pulse pressure amplification differed by diabetic status. In patients with diabetes, the use of blockers of the renin angiotensin system (which was more common in this population) and the E/E’ ratio were determinants. In the those without diabetes, they were family history of coronary heart disease and mean arterial pressure.
In this study, central and peripheral blood pressures were similar at baseline in the patients with hypertension plus diabetes or no diabetes. A positive relation was found between arterial stiffness and diastolic dysfunction in the total population. Pulse pressure amplification was inversely related to diastolic dysfunction only in patients with diabetes, with the E/E’ ratio contributing to 14% of the variance in amplification in these patients. Addressing the relation between arterial and cardiac function could be of value.