





An online risk prediction tool has been created to estimate the 2-year risk of a cardiovascular (CV) event in patients with type 2 diabetes (T2D) and diabetic nephropathy. The tool was developed by Jean-Pierre Fauvel, MD, CHU Lyon, Hôpital E. Herriot, Lyon, France, and colleagues, using data from the ALICE-PROTECT study, to improve treatment of patients with diabetic nephropathy.
The prospective, observational ALICE-PROTECT study included patients with T2D and proteinuria with an estimated glomerular filtration (eGFR) rate >15 ml/min/1.73 m2. The primary outcome was the number of patients at 2 years who reached the goal of a blood pressure <130/80 mmHg and proteinuria <0.5 g daily [Joly D et al. Diabetes Res Clin Pract 2015].
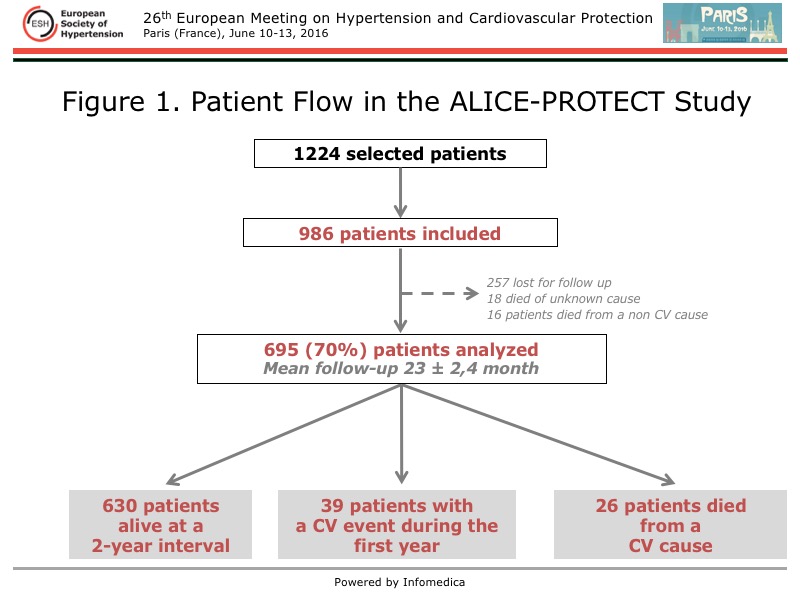
The mean age of the 986 patients in ALICE-PROTECT was 70 years, mean eGFR was 42 ml/min/1.73 m2, and 66% of patients had proteinuria >1 g daily. The flow of the study patients is shown in Figure 1.
{kind=link}
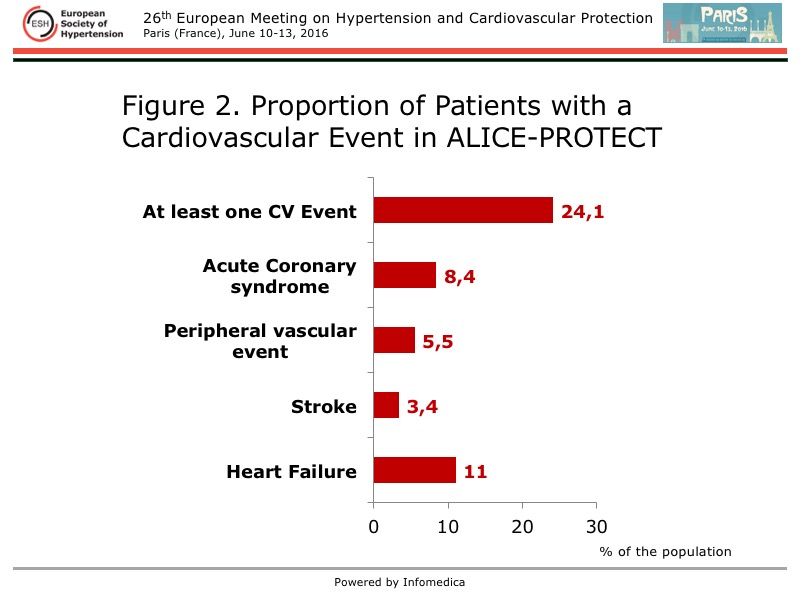
The proportion of patients who had a CV event during the 2-year follow-up of ALICE-PROTECT is illustrated in Figure 2.
{kind=link}
Fauvel and colleagues conducted the present analysis to create a Bayesian model to predict the global probability of CV events based on a range of scenarios in a manner that aligns with how physicians think. The variables included in the analysis were:
- Patient Characteristics
- Age, sex, body mass index, blood pressure, ethnicity, smoking habits
- Medical History
- Stroke, sleep apnea, peripheral arterial disease, ischemic heart disease, heart failure, diabetes duration, hypertension duration, retinopathy
- Biology
- eGFR, potassium, low-density lipoprotein cholesterol. HbA1c, proteinuria, hemoglobin
- Treatment
- Renin angiotensin system blockers, ASE, insulin, statin, diuretics, antithrombotic agent
Using the tree augmented naive algorithm to increase the robustness of the model, they created a Bayesian network that was a new model to simulate data, using the original data from the ALICE-PROTECT study. The area under the curve (AUC) was 71.6% for the receiver operator curve (ROC) when using the original dataset of the 695 patients who had a CV event during the study. The simulation was calibrated with 2000 simulated individual data, 1000 with and 1000 without a CV event. Multiple links between variables were found.
The results of their analysis revealed a 10-fold cross validation of their model of 70.8% for the AUC under the ROC. The AUC under the ROC was 74% for the original dataset of 695 patents. The sensitivity of the model was 64% and specificity 69.9%. The positive and negative predictive values were 84.2% and 43.7%, respectively.
Notably, the 2-year risk of a CV event can now be determined for an individual patient using an online calculator created from this work. The online calculator can be accessed at: https://www.hed.cc/?s=cvevent&t=CV%20Event The management of diabetic nephropathy can be optimized with this risk calculation.
The benefit of such a Bayesian network is the capacity to mimic the usual medical thinking of physicians and to analysis a large number of variables, with no a priori hypothesis. Fauvel noted such models can be created despite missing values, and that their robustness is enhanced by calibrating simulated data. Increasingly, these models are used as diagnostic tools for medical decision making.